Pramod Gupta, Atul Khare and Guru Reddy
Unicycive Therapeutics, Los Altos, CA, USA
Abstract
Objectives
Over 40% of dialysis patients have above-target phosphate. The efficacy and safety of oxylanthanum carbonate (OLC), a novel phosphate binder that forms the same insoluble phosphate complex as lanthanum carbonate, were assessed in two animal models.
Methods
Three groups of nephrectomized cats (n = 4 per group) received 0.0466 g OLC/kg body weight, 0.233 g OLC/kg body weight, or placebo. Six groups of rats (n = 6 per group) received placebo or 0.049, 0.099, 0.197, 0.394 or 0.788 g OLC/day. Endpoints included phosphate concentrations (urine, faecal and plasma) and serum lanthanum concentrations. All animals were observed for tolerance, injury and mortality.
Key Findings
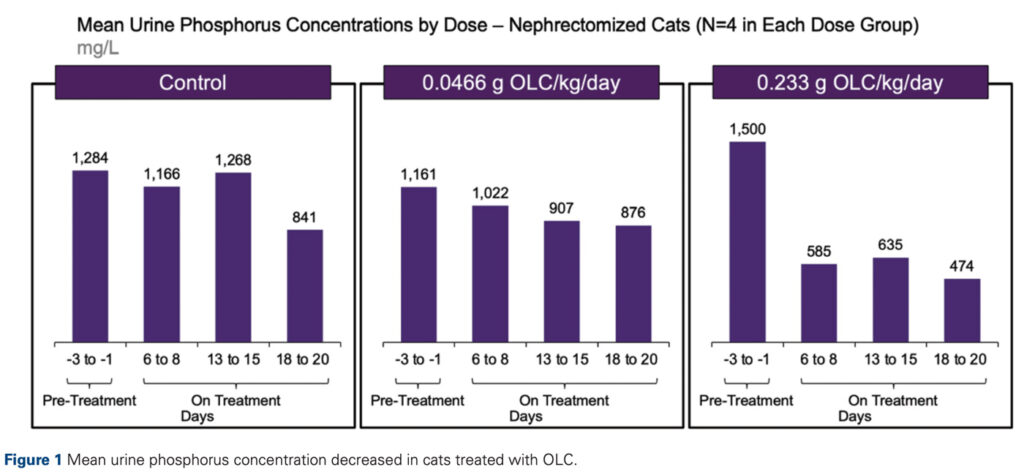
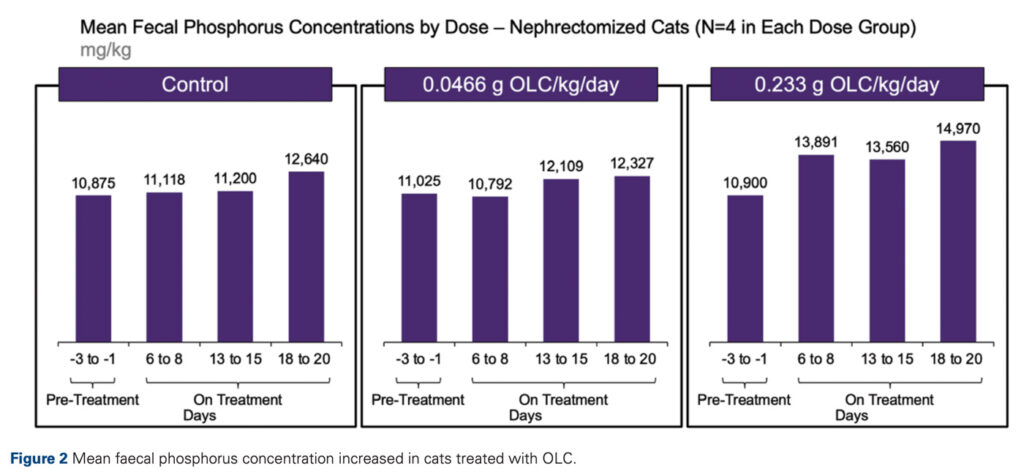
In cats, urine phosphorus concentrations decreased across treatment groups and faecal phosphorus excretion increased in higher dose groups compared to control and lower dose groups. A clear but non-significant decline in plasma phosphate was observed. In rats, urine phosphorus concentrations also decreased in all groups. The majority of serum lanthanum concentrations for rats in treatment groups were not significantly different from those in control groups. The study drug was well tolerated in both models.
Conclusions
OLC was effective for phosphate management and efficacy may be dose dependent. OLC was safe and well tolerated, indicating that it should be evaluated in the target population of patients with hyperphosphatemia.
Keywords
oxylanthanum carbonate; phosphate binder; chronic kidney disease; end-stage renal disease; hyperphosphatemia

Introduction
Approximately 37 million and 800000 people in the United States with chronic kidney disease (CKD) and end-stage renal disease (ESRD), respectively, are at risk of elevated phosphate, which increases as kidney function declines.[1] A study found that each 1 mg/dL increase in serum phosphate was associated with an estimated 23% increased mortality risk in CKD patients,[2] so achieving and maintaining adequate phosphate control is a crucial part of CKD and ESRD treatment. However, 43.1% of dialysis patients had a most recent phosphate concentration >5.5 mg/dL and 71.2% were >4.5 mg/dL.[3] This widespread lack of phosphate control is a critical challenge that must be addressed to improve clinical outcomes in CKD and ESRD patients.
The only pharmacological option for managing elevated phosphate is phosphate binders, which reduce the quantity of dietary phosphate that can be absorbed by forming insoluble compounds in the gastrointestinal (GI) tract. Over
80% of dialysis patients are prescribed binders,[4] yet large proportions do not achieve recommended phosphate levels, suggesting that available binders have suboptimal efficacy. Additionally, phosphate binders often require patients to ingest large volumes of medication several times a day and can cause adverse GI effects, both of which likely decrease treatment adherence, thereby negatively impacting efficacy. Inability to tolerate phosphate binders was cited as the reason for treatment discontinuation in 10% of patients.[5] Of these, almost 50% were due to GI upset.[5] There are also safety concerns associated with calcium-based binders, which have been linked to progressive coronary artery and aortic calcification.[6] Thus, there is a clear unmet need for a phosphate management therapy that not only achieves and maintains recommended target phosphate concentrations but is also easy to ingest, well tolerated and safe.
Oxylanthanum carbonate (OLC) is a novel phosphate binder that contains the same active moiety lanthanum and forms the same insoluble phosphate complex (lanthanum phosphate) in the GI tract as the approved lanthanum carbonate, which has the highest binding capacity of currently available binders.[7] Oxylanthanum carbonate is formulated as a tablet taken with water, and fewer GI adverse effects are expected due to the presence of a single carbonate moiety. We
present pharmacological data from two animal models that assessed the efficacy and safety of OLC.
Materials and Methods
Nephrectomized cat model
The efficacy and safety of OLC were assessed in nephrectomized cats. Twelve cats (five male and seven female) that successfully underwent a two-stage partial renal ablation procedure were split into three groups (four cats per group), with one control group and two treatment groups. From Day –5 to 20, all groups were fed a standard commercially available wet cat diet with low phosphorus and protein. Beginning on Day 0, 0.0466 g OLC/kg body weight (1Å~ dose level) and 0.233 g OLC/kg body weight (5Å~ dose level) was administered once daily in the morning to Groups 2 and 3, respectively, mixed with the predetermined individual food ration.
Two whole blood samples were collected from the jugular vein of each animal on Days –2, –1, 8, 15 and 20: a 1.3 ml sample into a tube containing lithium heparin anticoagulant; a 5.0 ml sample into a tube containing EDTA anticoagulant. Within 90 min of collection, blood samples were centrifuged at 3000 g for 15 min in a refrigerated centrifuge (4ÅãC at Jouan centrifuge BR 4i, rotor 540). Plasma was removed into plain tubes and shipped to certified laboratories in styrofoam boxes with ice packs (samples for phosphorus, calcium, urea and creatinine) or on dry ice (samples for parathyroid hormone [PTH]) for analysis using standard assays. Plasma phosphorus, calcium, urea and creatinine were analysed at the Clinical Laboratory at Charles River Laboratories BioLabs in Glenamoy, Ireland. Plasma PTH analysis was performed at Cambridge Specialist Laboratory Services in Cambridge, UK.
Urine samples were collected on Day –3, –2, –1, 6, 7, 8, 13, 13, 15, 18, 19 and 20. The volume of each 24-h urine sample was recorded. Feces were collected on the same days and the quantity (weight) of each 24-h sample was recorded. Faeces were stored at or below –20ÅãC until dispatched on dry ice to LUFA Nord-West for analysis of phosphate levels.
Body weights were recorded pre-treatment (Days –5 and –1) and during treatment (Days 8, 15 and 20). Tolerance observations including lethargy, vomiting, salivation, diarrhoea, tachypnoea, dyspnoea, pruritis, and ataxia were recorded on Study Days 0, 8, 15 and 20.
Efficacy was assessed using urine, faeces and plasma phosphate levels pre-treatment (Days –3, –2 and –1) and during treatment (Days 6, 7, 8, 13, 14, 15, 18, 19 and 20). Renal function was monitored using plasma calcium, PTH, urea and creatinine concentrations pre-treatment (Day –2) and during treatment (Days 8, 15 and 20).
Rat model
The efficacy and safety of OLC were also evaluated in rats. Thirty-six male SD-HLA (SD) CVF rats with jugular vein cannulae were randomly assigned to control and treatment groups (six rats per group) and were treated for a total of seven consecutive days (Days 3–9). Group 1, the control group, received a vehicle diet. Groups 2, 3, 4, 5 and 6 received 0.049, 0.099, 0.197, 0.394 and 0.788 g OLC/day, respectively.
Blood samples for determination of serum phosphorus and creatinine concentrations (sampling volume approximately 300 μl) were collected approximately 3–4.4 h post-dose on Days 1–11. Blood samples for determination of serum lanthanum concentrations (sampling volume approximately 900 μl) were collected on Days 3 and 9 only. The animals had access to drinking water and food prior to sample collection. Blood samples were taken via the jugular vein or jugular vein cannula. Samples were collected on ice, protected from light, into gel microtainers containing no anticoagulant and centrifuged for serum preparation. Urine was collected on wet ice prior to daily diet administration at 24-h intervals from Day –2 to 11 for the determination of phosphorus and creatinine concentrations. Urine and serum samples for phosphorus and creatinine analysis were sent to the Clinical Chemistry Department at MPI Research in Mattawan, MI and analysed using an Olympus AU600 Clinical Chemistry Analyzer (USA). Samples for serum lanthanum analysis were sent on dry ice to Exygen Research, Inc. (State College, PA, USA) for analysis using inductively coupled argon plasma mass spectrometry (ICP-MS, Elan 6000, Perkin Elmer Sciex, USA).
For safety, all animals were observed for mortality, morbidity, injury and the availability of food and water twice daily. Body weights were measured before randomization on Day –2 and then once daily prior to diet administration beginning on Day –1. Food consumption was measured daily beginning on Day –2, and food efficiency and test article consumption were calculated. Animals that died during the study received complete necropsy examinations.
Efficacy endpoints included urine concentrations of phosphate, creatinine, and phosphate/creatinine ratio, and serum concentrations of phosphate, creatinine, phosphate/creatinine ratio and serum lanthanum.
Descriptive statistics consisted of means with a 95% confidence interval, standard deviations, standard errors of the mean and n values. For each endpoint and time period, an analysis of variance (ANOVA) was performed using treatment as an effect. If statistical significance (P < 0.05) was found, then follow-up analyses were conducted using Group Pair-Wise analysis procedures. Statistical analyses were conducted using SAS.
Results
Nephrectomized cats
In the nephrectomized cat study, urine phosphorus concentrations decreased for all animals in the treatment groups during OLC treatment compared to pre-treatment. Mean urine phosphorus concentrations decreased by 285 mg/l (1161 mg/l pre-treatment to 876 mg/l) and 1026 mg/l (1500 mg/l pre-treatment to 474 mg/l) in the 0.0466 g OLC/kg/day and 0.233 g OLC/kg/day groups, respectively (Figure 1).
Figure 1.
Faecal phosphorus excretion increased during treatment for cats in the higher dose group compared to the control and lower dose group (Figure 2). Mean phosphorus increased by 2800 mg/kg dry matter (10 900 mg/kg dry matter to 13 700 mg/kg dry matter), 275 mg/kg dry matter (11 025 mg/kg dry matter to 11 300 mg/kg dry matter) and 1475 mg/kg dry matter (10 875 mg/kg dry matter to 12 350 mg/kg dry matter) in the 0.233 g OLC/kg/day, 0.0466 g OLC/kg/day and control groups, respectively.
Figure 2.
When phosphate concentrations were plotted as a percentage of pre-treatment concentrations, a clear but nonsignificant decline in plasma phosphate was observed (P = 0.335 and 0.066 for the 0.0466 g OLC/kg body weight 0.233 g OLC/kg body weight groups, respectively).
One adverse event consisting of one animal in the 0.233 g OLC/kg/day group with clear and watery vomit on Day 0 was observed, but no diet was visible in the vomit. There was no overall difference for mean plasma urea and creatinine values between dose groups. All cats in all groups had normal levels
for plasma phosphate and calcium throughout the study. All cats gained or maintained weight during the study.
Sprague Dawley rats
In the rat study, urine phosphorus concentrations decreased in all groups during treatment. Mean urine phosphorus concentrations dropped by 0.1, 2.3, 3.0 and 3.5 mg/day in the control, 0.197, 0.394 and 0.788 g OLC/day groups, respectively. On Day 7, mean serum phosphorus concentrations were generally lower in the treatment groups than in the control group, with –10%, –25%, +3% and –21% change from baseline in the control, 0.197, 0.394 and 0.788 g OLC/day groups, respectively. The majority of serum lanthanum concentrations for animals in the treatment groups were not significantly different from those in control animals.
With the exception of the 0.099 g OLC/day dose group, mean body weights decreased by the end of the study. The decrease in body weight was highest in the control group (~5% relative to pre-study mean weight). The number of unscheduled deaths was 2, 1, 2 and 0 in the control, 0.099, 0.394, and 0.788 g OLC/day groups, respectively. The deaths occurred randomly, unrelated to treatment.
DISCUSSION
The ultimate goal of phosphate management is to achieve and maintain phosphate concentrations within the recommended, and ideally normal, range to avoid the negative outcomes associated with hyperphosphatemia. However, real-world data show that currently available binders do not consistently maintain and achieve recommended phosphate concentrations.[8] Characteristics of binders that negatively impact the treatment experience for patients (e.g. GI adverse effects[5]) and established safety issues associated with calcium-based phosphate binders[6] may decrease adherence, thereby decreasing efficacy. Thus, there is an unmet need for a treatment that effectively controls phosphate while being safe and well tolerated.
This publication presents efficacy, safety and tolerability data from the first two pharmacological studies of the novel compound OLC, which can potentially provide the same phosphate-binding capacity as current therapies with a lower dose and is expected to cause fewer GI adverse events. Based on urine phosphorus concentrations, faecal phosphorus excretion, and serum phosphorus concentrations, OLC effectively decreased phosphate absorption. The overall consistent results across multiple endpoints and both animal models provide strong support for the efficacy of OLC. The efficacy of OLC may be dose-dependent, which would allow for the dose to be titrated up in patients with phosphate levels that are difficult to control. Oxylanthanum carbonate was safe and well tolerated in both animal models, indicating that it should be evaluated in human trials.
These studies had some limitations. First, results from animal studies may not directly translate to humans. However, preclinical animal studies are an important, established part of new drug research, and allometric scaling is widely used during drug discovery and development to predict pharmacokinetic interactions in humans based on preclinical animal datasets.[9] Another limitation was that the treatment period in the rat study was relatively short (seven days), but this is consistent with other animal studies.[10]
Based on these two pharmacological studies, OLC demonstrated good efficacy and safety and should, therefore, be evaluated in human trials. Increased safety and tolerability may also increase adherence, which would lead to more consistent phosphate control to recommended concentrations. The more phosphorus values do not exceed 4.5 mg/dL, the better chance of survival,[11] so improved phosphate control would decrease mortality risk. Thus, if approved, OLC will be a welcome option for patients that has the potential to not only improve efficacy but also increase the quality of life.
CONCLUSIONS
Overall, OLC was effective for phosphate management. Administration of OLC to nephrectomized cats and healthy rats resulted in the reduction of urinary phosphate excretion. In cats, there was a corresponding increase in faecal phosphate excretion, and rats saw a decrease in serum phosphate concentrations. There was evidence that efficacy is dosedependent. Oxylanthanum carbonate was safe and well tolerated in animal models, indicating potential for future studies in humans.
Author Contributions
Pramod Gupta, Atul Khare and Guru Reddy contributed to the study design, data acquisition and data analysis. Pramod Gupta, Atul Khare and Guru Reddy all contributed to and approved the final manuscript.
Funding Sources
This study was funded by Unicycive Therapeutics, Inc.
Conflict of Interest Statement
Pramod Gupta, Atul Khare and Guru Reddy are employees of Unicycive Therapeutics, Inc.
Statement of Ethics
The protocol for the nephrectomized cat study was approved by the Ethics Committee of Charles River Laboratories Biolabs Europe on 8 September 2005 (study number USA007/05-001). The protocol for the Sprague Dawley rat study was approved by MPI Research, which is fully accredited by the Association for Assessment and Accreditation of Laboratory Animal Care International (AAALAC International), on 19 March 2004 (study number 1071-001).
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References:
- Isakova T, Wahl P, Vargas GS et al. Fibroblast growth factor 23 is elevated before parathyroid hormone and phosphate in chronic kidney disease. Kidney Int 2011; 79: 1370–8. https://doi.org/10.1038/ki.2011.47
- Kestenbaum B, Sampson JN, Rudser KD et al. Serum phosphate levels and mortality risk among people with chronic kidney disease. J Am Soc Nephrol 2005; 16: 520–8. https://doi.org/10.1681/ASN.2004070602
- Serum phosphorus (most recent), categories: DOPPS Practice Monitor, 2022. https://www.dopps.org/DPM-HD/Files/phosphmgdl_c_overallTAB.htm.
- Phosphate binder use, last 3 months: DOPPS Practice Monitor, 2022. https://www.dopps.org/DPM-HD/Files/maxPBINDER_use_c_overallTAB.htm.
- Wang S, Anum EA, Ramakrishnan K et al. Reasons for phosphate binder discontinuation vary by binder type. J Ren Nutr 2014; 24:105–9. https://doi.org/10.1053/j.jrn.2013.11.004
- Chertow GM, Raggi P, Chasan-Taber S et al. Determinants of progressive vascular calcification in haemodialysis patients. Nephrol Dial Transplant 2004; 19: 1489–96. https://doi.org/10.1093/ndt/gfh125
- Daugirdas JT, Finn WF, Emmett M et al; Frequent Hemodialysis Network Trial Group. The phosphate binder equivalent dose. Semin Dial 2011; 24: 41–9. https://doi.org/10.1111/j.1525-139X.2011.00849.x
- Serum phosphorus (3 month average), categories: DOPPS Practice Monitor, 2022. https://www.dopps.org/DPM-HD/Files/meanphosphmgdl_c_overallTAB.htm.
- Valic MS, Zheng G. Research tools for extrapolating the disposition and pharmacokinetics of nanomaterials from preclinical animals to humans. Theranostics 2019; 9: 3365–87. https://doi.org/10.7150/thno.34509
- Katai K, Tanaka H, Tatsumi S et al. Nicotinamide inhibits sodiumdependent phosphate cotransport activity in rat small intestine. Nephrol Dial Transplant 1999; 14: 1195–201. https://doi.org/10.1093/ndt/14.5.1195
- Lopes MB, Karaboyas A, Bieber B et al. Impact of longer term phosphorus control on cardiovascular mortality in hemodialysis patients using an area under the curve approach: results from the DOPPS. Nephrol Dial Transplant 2020; 35: 1794–801. https://doi.org/10.1093/ndt/gfaa054