Atul Khare1, PhD; Pramod Gupta1, PhD
1Unicycive Therapeutics, Inc., Los Altos, CA
Background
- ~600k kidney failure patients in the US undergo dialysis1
- Due to poor kidney function, patients often have hyperphosphatemia, which leads to an increased risk of death2
- Patients usually rely on dietary restriction and phosphate (P) binders to avoid hyperphosphatemia
- Current P binders often do not achieve normal levels of P3 and have a high pill burden due to large and high quantity of pills4,5
- A therapeutic option with a potentially smaller dose volume (i.e., fewer pills and smaller pill size) and efficacy similar to or possibly better than current products may enhance patient quality of life (QoL)
- Lanthanum dioxycarbonate, Renazorb (LDC), is a novel nanotechnology product that combines lanthanum, which has the highest binding capacity vs. other P binders, with a potentially smaller pill size that is swallowed with water rather than chewed

OBJECTIVE
We present results of a phase 1 study evaluating LDC’s P binding capacity and tolerability
Methods
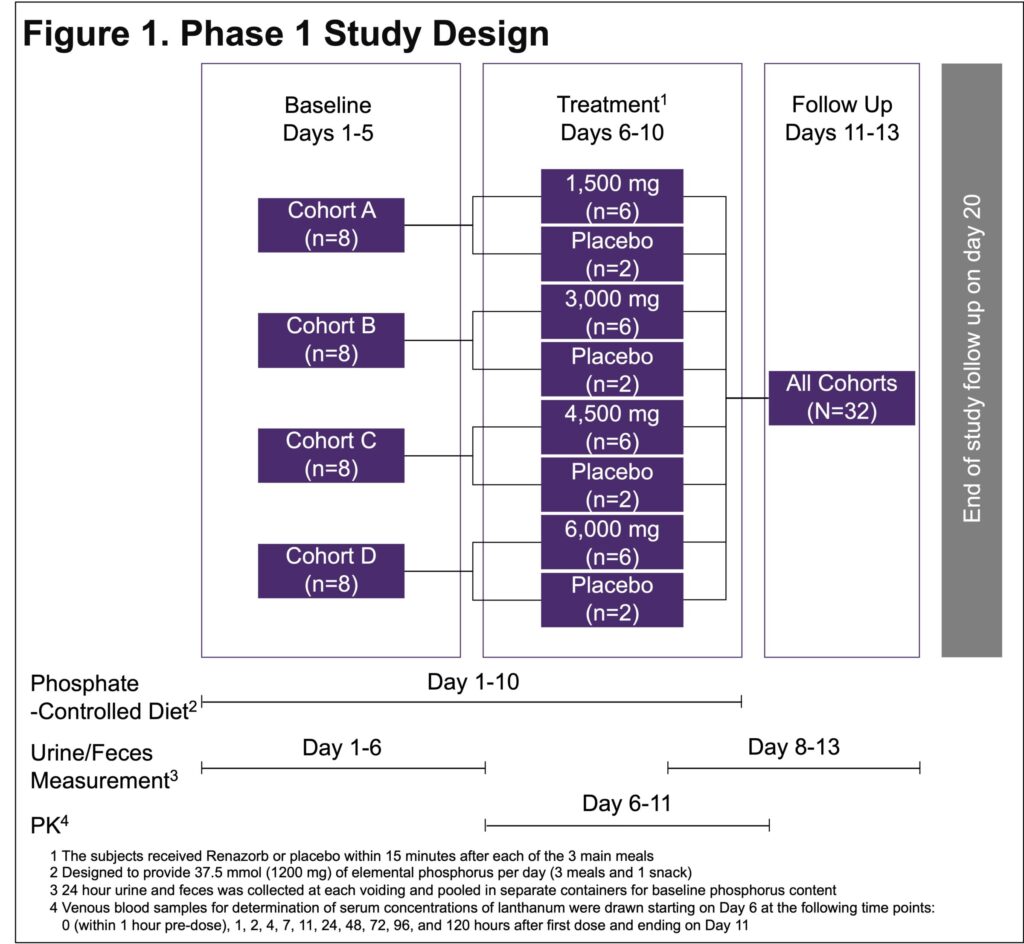
- A phase 1, double-blind, placebo-controlled study evaluated LDC’s P binding capacity and tolerability in 4 cohorts of 8 healthy adults
- 4 separate LDC doses of 500 mg tablets were administered after meals for 5 days: 1,500, 3,000, 4,500, and 6,000 mg/day (Figure 1)
Results
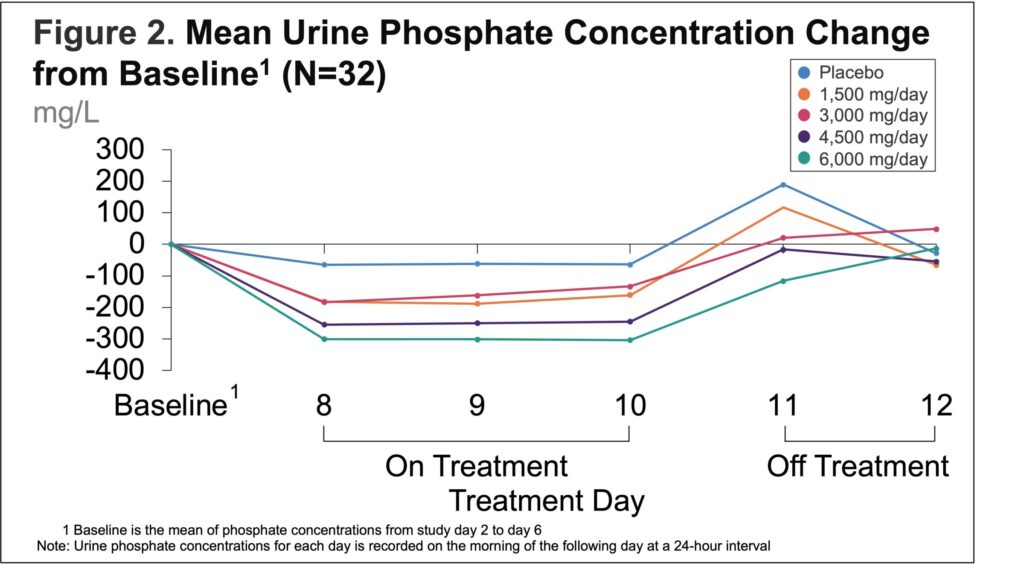
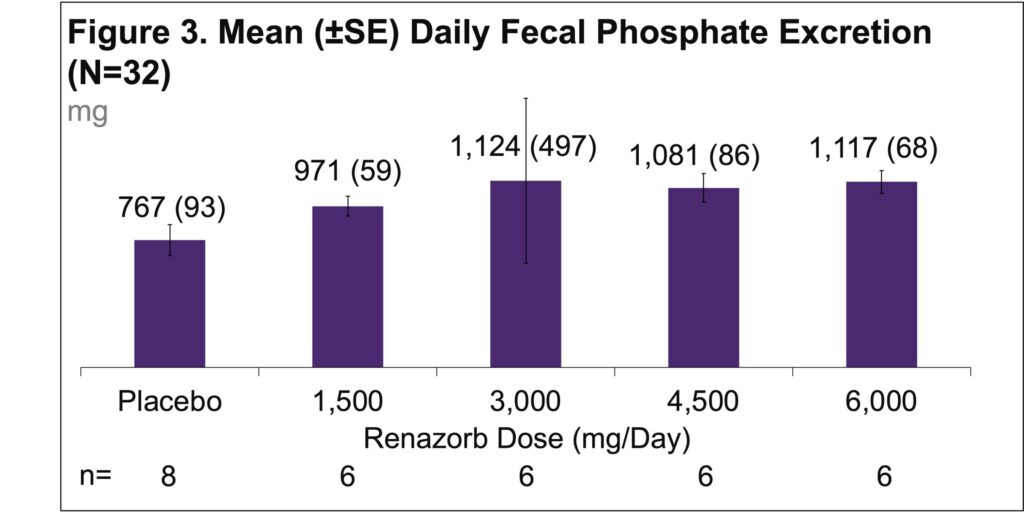
- All doses reduced the amount of P excreted in urine and increased the amount excreted in feces (Figure 2 & 3)
- Mean overall change in P excretion showed a statistically significant dose-response trend
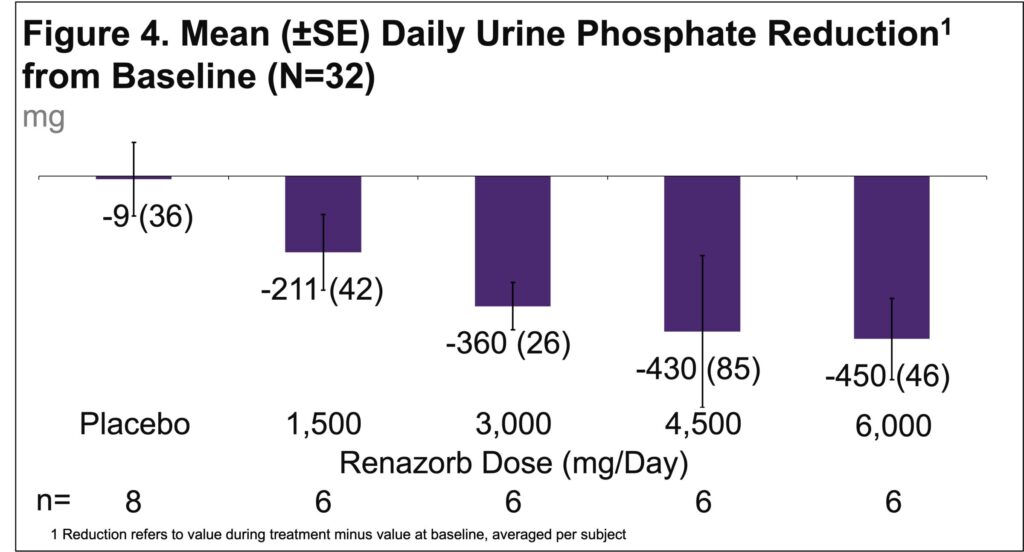
- Higher doses of LDC are associated with higher urine phosphate excretion (Figure 4)
- LDC showed significant mean reduction in urine P excretion with 1,500 mg/day, 3,000 mg/day, 4,500 mg/day, and 6,000 mg/day dose (Figure 4)
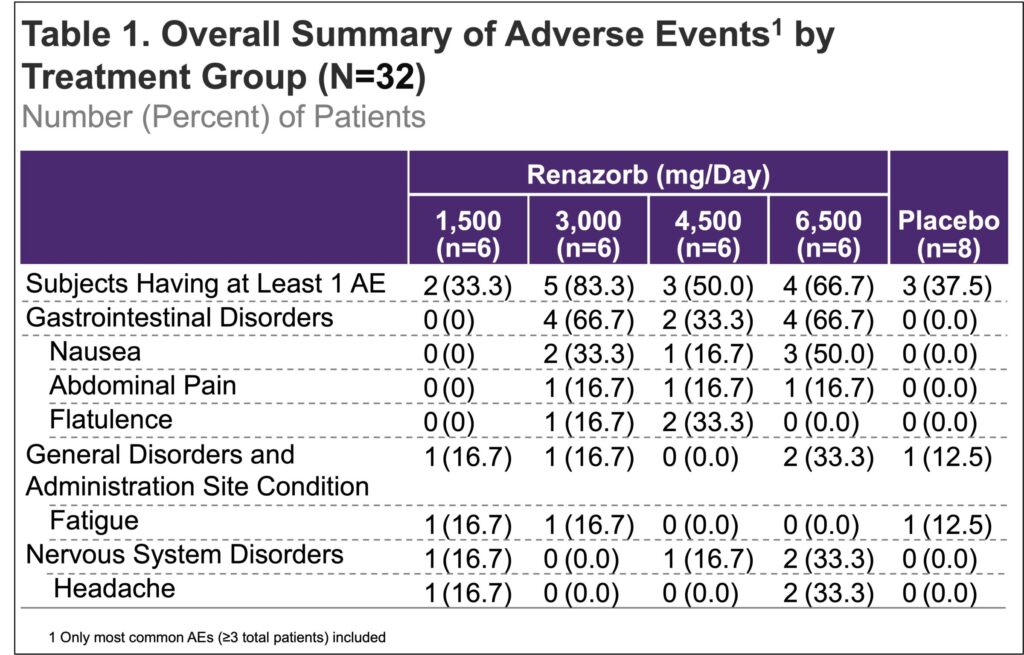
- There were no severe or life-threatening AEs, serious AEs, deaths, or AEs leading to discontinuation (Table 1)
CONCLUSIONS
- LDC was effective in binding to dietary P, and the efficacy was dose-proportional
- LDC was well tolerated
- LDC may be a welcome choice for patients as it is effective and is a small swallowable pill
IMPLICATIONS
- Potential benefits of LDC may include reduced pill burden and ease of dose administration (smaller easy-to-swallow vs. chewable), which collectively has the potential to increase patient adherence, improve treatment outcomes, and enhance QoL
References:
1. USRDS. USRDS Annual Data Report. 2020.
2. Chang AR, et. al., Am J Kidney Dis. 2014.
3. DOPPS. DOPPS Practice Monitor. 2021.
4. Chiu YW, et. al., Clin J Am Soc Nephrol. 2009.
5. Arenas MD, et. al., Nefrologia. 2010.
Acknowledgments:
Writing support was provided by Xelay Acumen Group, Inc., and funded by Unicycive Therapeutics, Inc.